
Archive for September, 2014
New Marathon Record: An Analysis & Next Steps
On Sunday September 28, 2014 the Kenyan runner Dennis Kimetto ran the marathon in 2 hours 2 minutes and 57 seconds breaking the record of 2:03:23 set last year on the same course. Starting in 2007 with Haile Gebrselassie’s 2:04:26 the record has been broken five times, all at Berlin.
What is Physiologically “Possible”?
Back in 1991, I created a predictive model of marathon performance based on well-established physiological variables. I then asked what would happen to the marathon world record if the same athlete had optimal values for all of the key variables associated with distance running success. The predicted time I came up with for such a superman was just under 1:58:00. The model, plus some speculation, was revisited in 2011 with my colleagues Alejandro Lucia and Jonatan Ruiz and we projected that someone might break 2 hours by sometime between about 2025 and the late 2030s. So, what seemed inconceivable to many in 1991 seems to be getting closer by the year.
What Might Happen Soon?
Many elite distance runners have marathon personal bests that are about 4.6 or 4.7 times their 10k personal bests (a marathon is ~42.2k). If you use this rule of thumb then the current world record for the 10k (26:17:53) works out to a predicted marathon time somewhere between just under 2:01and about 2:03:25. Similar values emerge using various point tables and race conversion calculators. So, the current record is perhaps still a bit on the “slow” side, and I would not be surprised if the record fell by another minute or so in the next few years.
How to Make it Happen Sooner
If I were a race promoter, shoe company, or billionaire interested in wanting to get the marathon record as fast as possible as soon as possible, here are three things I would do:
- A lot of the top runners decide where they are going to run and who they are going to run against based on financial considerations. You can only run so many fast marathons per year so it is important for top runners to make each one a pay day. To get more of the top people in the same race, I would offer purses to be split by all runners under specified split times at say the half-way point, 30k, 35k, and 40k. This sort of pay out structure would encourage the top people to work together, draft, and it would not penalize risk taking if someone went out too fast and then faded. I would start with split times based on 2:02:30 and work down as records fell.
- Develop a 5 or 8k loop that was flat and had an ideal surface and then stage a yearly “elites only” race on that course. Pick a part of the world and time of the year where weather conditions are likely to be ideal with low humidity and temperature about 10C (50F).
- Run the race in the late afternoon as the sun is setting. There is some anecdotal evidence that this might be an ideal time vs. the early morning.
2:02 or Bust
When colleagues, fans and members of the media ask me what I think might happen, I tell them that something under 2:02 is possible now and that once the record gets below 2:02 the fun will begin.

Jens Voigt & Ideas About a “Fairer” Triathlon
Last week the 43 year old cyclist Jens Voigt set a world record for the 1 hour ride. Voigt covered 51.115 kilometers and then retired. Voigt has had a long career near the top of professional cycling and avoided the doping scandals that have plagued cycling over the last several decades.
What Does Voigt Have to do With Triathlons?
The short answer is not much. Normally a performance like this is a lead into a discussion about aging, the history of world records, the role of technology in sports (he used an aero bike), or some other element of sports physiology. However, Voigt’s record got me thinking about what would happen if each element of a triathlon was designed to take about the same amount of time. Both the Olympic distance Tri (1.5k swim, 40k ride, and 10k run) and the Ironman distance Tri (2.4 mile swim, 112 ride, and 26.2 mile run) have bike segments that take about 50% or more of the total time for elite competitors. The swim segment also takes less time than the run for elites.
Three 1 Hour Segments?
So, what would happen if there was a triathlon designed around world records for the hour? The current world record for the hour run is just over 21km by Haile Gebrselassie. The best record I could find for the hour swim is 6135 yds (about 5610 meters) set by Robert Margalis in a 25 yard pool in 2007. The swimming record, while impressive, is likely soft in comparison to the cycling and running records that were set by truly world class athletes in their respective disciplines.
Based on these records (and some other back of the envelope calculations) perhaps something with a running distance about 3.8 times the swim distance would equalize those two triathlon elements. A biking distance perhaps 2.5 times the running distance would also seem reasonable. So how about a swim just over 5k, a 50k ride, and 20k run? These ratios are a start. To do this well one would need a detailed statistical analysis of a larger number of elite performances, but my guess is that such an analysis would lead to ratios and distances similar to the ones I have suggested.
Take it Indoors?
Why not also take it indoors and come up with something like the triathlon version of the Crash-B Sprints for rowing. These races are conducted indoors on rowing ergometers and a number of winners and record holders have impressive records on the water.
For the Triathlon the format might be an hour swim in a short course pool and distance run in an hour on a calibrated treadmill. The trick would be how to deal with the bike element indoors. I would use some measure related to average watts of power output per kg of body weight over the hour. I have seen varying reports of what Voigt did, but it appears that he averaged about 400 watts per minute. This works out to a bit more than 5 watts per kg.
Using the ratios I mentioned above, point scales and records could be established for each discipline. Perhaps a top score for each event would be worth 1,000 points. Such a scale could also be age and sex adjusted so performances could be easily compared for each competitor. Perhaps things could be more strategic by letting each athlete pick their own preferred order of events with a standard 5 minute transition period between events. Would most people do the swim second to give their legs a break?
Just a Thought Exercise?
So far this is just a thought exercise or perhaps the beginning of a barroom argument for endurance athletes. However, I would be interested in hearing other thoughts about how this might be done and if anyone is interested in sponsoring such a competition it would be easy to formalize the ideas outlined in this post. Finally, I volunteer to be the first commissioner of the “Three Hour Test”.
Too Much Chess vs Too Much Exercise?
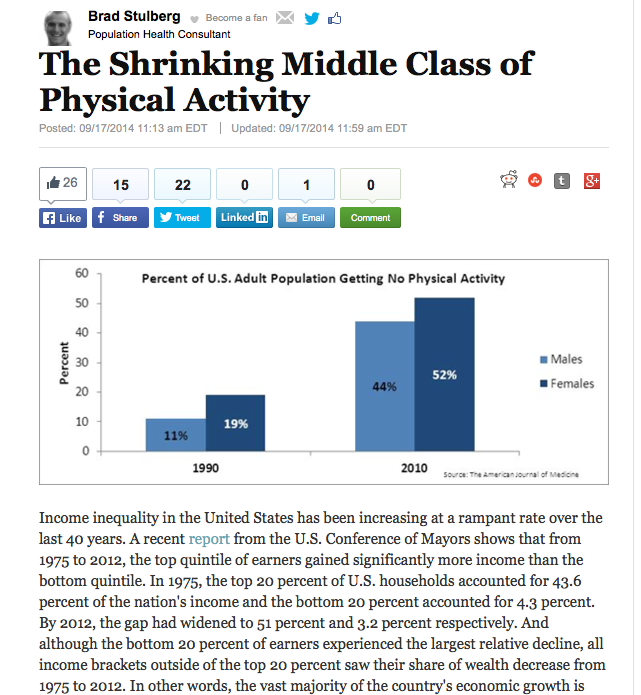
Last month the “too much exercise” story hit the media again. The general idea is that while moderate amounts of exercise reduce all-cause and cardiovascular mortality, those who really push it lose some of the protective effects of exercise and there is U or J shaped dose-response curve between exercise and health outcomes. This unproven idea suggests that mortality might actually start to rise for those who “exercise too much”.
The limitations of this story have been parsed and analyzed for the general public by people like Amby Burfoot, Alex Hutchinson, and Brad Stulberg. Additionally, a couple of years ago I did a piece on too much exercise that went over what the physiology does or does not say about this topic, and the short answer is that the physiology data tends to reject the whole idea. In other words people who exercise a lot into middle age and older tend to have big coronary arteries that can open wide and the pumping function of their hearts is excellent.
The recent papers and publicity also generated a long multi-faceted e-mail exchange with physician colleagues and writers interested in the topic. Some of the physicians are believers in the too much exercise hypothesis, others like me are skeptics. In the middle of the exchange I came across a headline in the Guardian about two deaths at the World Chess Olympiad. That led to an e-mail to the group titled “Too Much Chess” and several rounds of electronic trash talking.
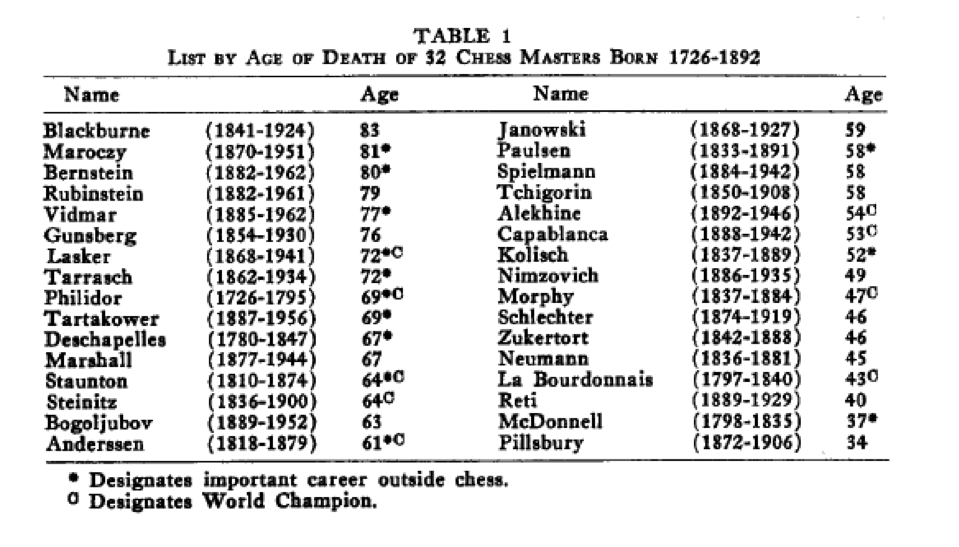
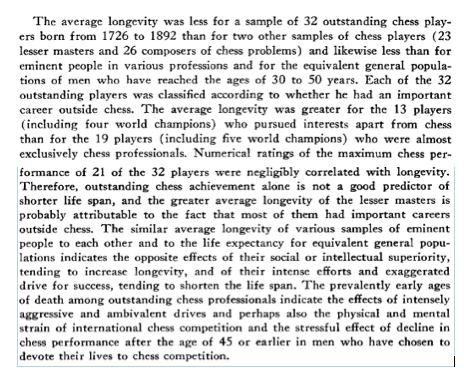
Not being able to help myself, I looked on PubMed, the superb electronic search engine for medical research papers maintained by the National Institutes of Health, for articles on longevity and Chess. I found one — from the late 1960s! Unfortunately there is no easy to download summary or full paper, but the table below is interesting as is the conclusion of the paper extracted below.
What to Make of the Data?
The first thing to note is that the table is a bunch of one off dates about various players. The second thing to note is that the total time frame of the cohort ranges from the 1700s up to the middle 1960s, a time that included all sorts of medical advances from ideas about basic sanitation, to vaccines and antibiotics. We also know nothing about what the cause of death was for the chess players or anything about other health behaviors like smoking or excessive drinking. The summary then goes on with some convoluted language about the relationship between social and intellectual superiority vs. the drive for success and longevity. So, there is not a whole to the chess and longevity story but some interesting factoids and speculation from the 1960s.
Why Do A Whole Lot of Anything?
When I read stuff about too much of this or too much of that, I wonder if all challenging activities in life (chess, sports, music, and art to name a few) have to have some sort of return on investment calculation. If so are the only acceptable outcomes improved odds of a longer life or perhaps some sort of financial reward? What about doing something because it is challenging, or you enjoy it? What about striving for excellence for its own sake? What about pushing your own limits for the sake of pushing your own limits? Also, who decides what is too much of what? At what level are we free to choose what we become, or will even more external norms be foisted on everyone? These are questions with no right or wrong answer, but in a world where we get pushed and pulled in all sorts of ways with return on investment thinking, it might be worthwhile to come up with your own answers.
Not every human activity needs to be justified, medicalized or financialized, some just need to be done for the sake of doing them.
Why Doctors Shouldn’t Be Sick of Their Profession
Last week the Wall Street Journal ran an essay titled “Why Doctors Are Sick of Their Profession.” It was authored by the cardiologist Sandeep Jauhar and based on is his book, Doctored: The Disillusionment of an American Physician. Numerous friends and colleagues have e-mailed me links to the piece for feedback and discussion.
The Highlights of the Essay
- Loss of respect and status since the golden age of American Medicine that Dr. Jauhar says occurred from 1940-1970. This era was also marked by rising life expectancy and the “conquest” of many diseases (at least in the developed world).
- Stagnant incomes and high med-school debt.
- Loss of autonomy, too much bureaucracy, burnout and the replacement of the simple private practice model with all sorts of other arrangements which are all linked.
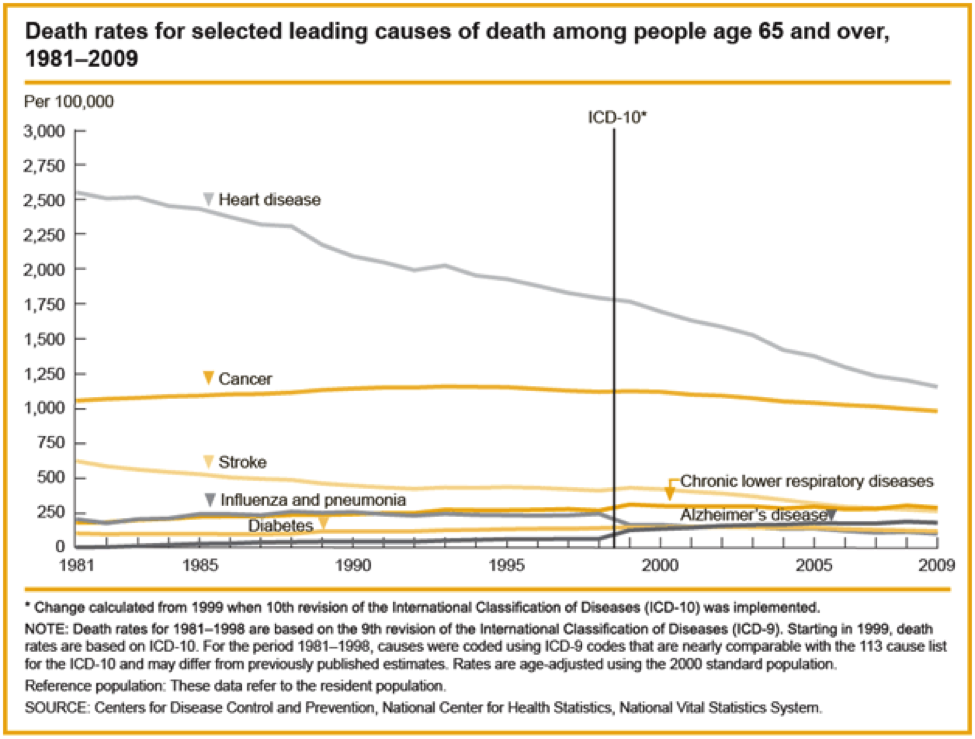
- He also mentions that the loss of morale is happening in spite of ongoing progress against many diseases. Deaths from heart disease and stroke for example have gone way down, and life expectancy continues to rise.
What Does the Data Say?
Below are three charts and a summary from a recent research article that touch on some of the issues raised by Dr. Jauhar.
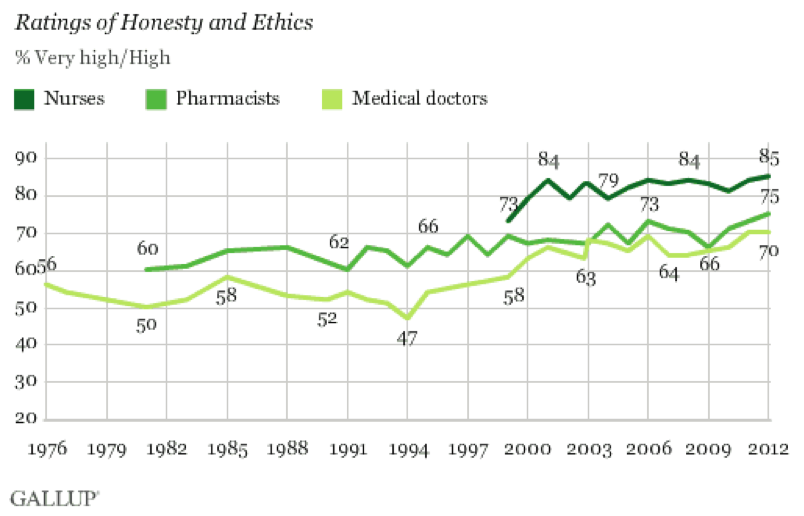
1) Respect: = The chart below shows some Gallup Poll data from 2012 demonstrating that respect for physicians seems to have risen over the last 35 or so years. Our colleagues in Nursing and Pharmacy do even better.
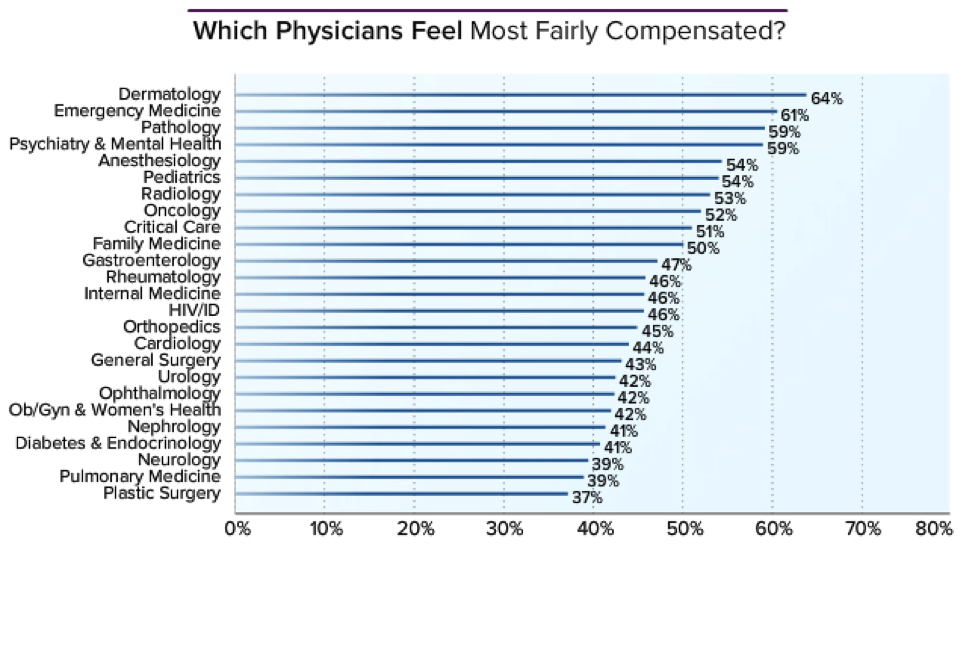
2) Income: The next chart shows that many physicians feel fairly compensated (the average is about 50%), and there does not seem to be a correlation between satisfaction. The chart comes from a comprehensive 2014 assessment via Medscape.com.
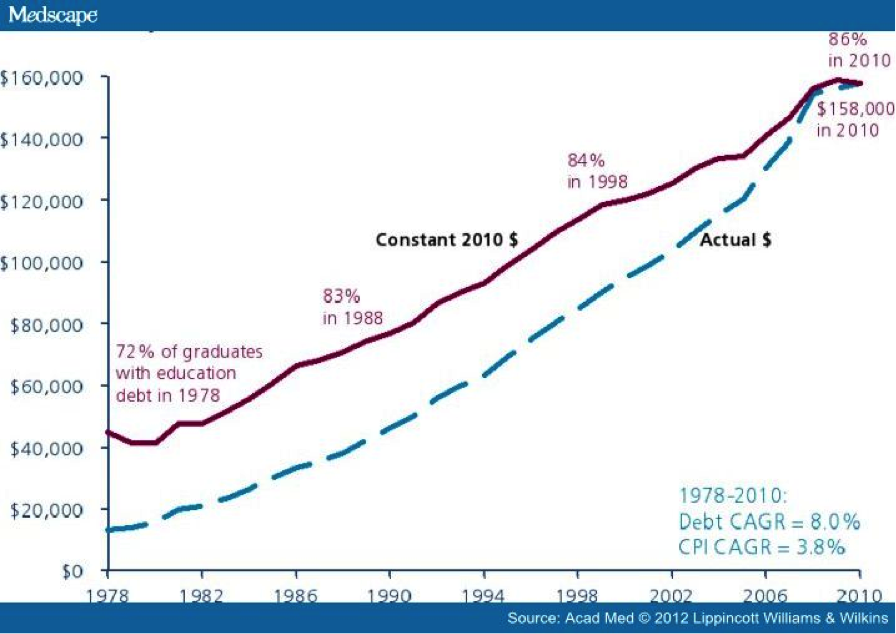
3) Debt: Anyway you slice things the med-school debt picture is bad and the trend lines are not good.
4) Burnout: Physician burnout does appear to be a problem compared to the general population.
“Results: Of 27 276 physicians who received an invitation to participate, 7288 (26.7%) completed surveys. When assessed using the Maslach Burnout Inventory, 45.8% of physicians reported at least 1 symptom of burnout. Substantial differences in burnout were observed by specialty, with the highest rates among physicians at the front line of care access (family medicine, general internal medicine, and emergency medicine). Compared with a probability-based sample of 3442 working US adults, physicians were more likely to have symptoms of burnout (37.9% vs 27.8%) and to be dissatisfied with work-life balance (40.2% vs 23.2%) Highest level of education completed also related to burnout in a pooled multivariate analysis adjusted for age, sex, relationship status, and hours worked per week. Compared with high school graduates, individuals with an MD or DO degree were at increased risk for burnout (odds ratio [OR], 1.36; P < .001), whereas individuals with a bachelor’s degree (OR, 0.80; P = .048), master’s degree (OR, 0.71; P = .01), or professional or doctoral degree other than an MD or DO degree (OR, 0.64; P = .04) were at lower risk for burnout.
Conclusions: Burnout is more common among physicians than among other US workers. Physicians in specialties at the front line of care access seem to be at greatest risk.”
My Take:
The issues above are very complex and they also vary by things like physician specialty, age, gender, and type of practice. However, I would offer the following general observations:
- In contrast to Dr. Jahaur’s assertion, respect for physicians has increased over the years.
- Medicine has never had more to offer patients. The recent reports of exciting new drugs for heart failure and high cholesterol are examples of the ongoing lifesaving innovation that happens all the time. Many operations that were once associated with high blood loss and blood transfusions are now bloodless. Importantly, there have been and are ongoing advances in almost every area of medicine including public health. Questions about how to deliver care fairly and effectively at a reasonable cost are major challenges, but I would rather be dealing with logistical questions than questions of basic efficacy. Dr. Jahaur could easily have painted a more optimistic picture and his essay only tells part of the story.
- The income data in Dr. Jahaur’s article is subject to all sorts of debate as the link associated with the income chart covers many of the nuances. Again Dr. Jahaur could easily have painted a more optimistic picture and his essay only tells part of the story.
- The Debt issue is a real problem and I see it influencing career choices of the med-students and young physicians I work with. If we want more generalist and primary care physicians it needs to be addressed. Fortunately, there are a number of ideas out there that might be explored to address this challenge.
- When I started med-school in 1982 people were just starting to talk about morale, work life balance, and burnout. Additionally, if you actually talk to people who practiced in the 1950s and 60s, they were perpetually on call, worked sometimes foolish hours, and had little back up. More importantly they will all tell you that in retrospect that they had little to offer patients. Most have more than one personal horror story about a terrible outcome that just would not happen today. Most would tell you it was not exactly the good old days. As is the case with debt there are solutions to things like the paper work and clerical burden leading to burnout. Additionally, with a little creativity it should be possible to keep the compliance burden under control with smart regulations. This would free up time for patients, ongoing learning, and other activities that might lead to increased professional satisfaction.
Summary
On the whole Medicine has never been better and the challenges confronting physicians are not insurmountable and many solutions have been adopted in various practices and are on the table elsewhere. As I pointed out several times above, Dr. Jahaur could easily have painted a more optimistic picture and his essay only tells part of the story. Finally, the information above clearly shows that many of his assertions are not backed by the data. Those that are can be fixed. I have seen vast progress in the last 32 years and hope I can see at least 32 more years of progress. Things are only getting better.
You are currently browsing the Human Limits blog archives for September, 2014.
LIKE MIKE

SUBSCRIBE TO RSS
